Kidney stone
The kidney stones are solid aggregates that can be formed in any part of the urinary tract. They originate as microscopic particles, but over time they grow becoming similar to stones.
The medical term that describes this condition is nephrolithiasis, which in Greek means stones in the kidney. The kidneys filter the blood and discharge waste matter in the urine. When these substances do not dissolve completely in the urine, “crystals” are formed, i.e. the initial microscopic nuclei from which the calculi are developed. Nearly always, the calculi are formed in the kidneys where they can remain without showing any symptom and so do not require any treatment.
Stones can migrate from the kidney to the ureter (the tube that carries urine from the kidney to the bladder): this step is the origin of the “renal colic” a severe pain that starts from the flank and radiates to the back or to the groin. A stone can also block the flow of urine, causing an increase in the pressure that affects the kidney causing an dilation called “hydronephrosis”.
The pressure increase causes stretching and subsequent contraction of the ureter, which is the origin of the mechanism of a severe pain.
Many kidney stones are able to pass spontaneously with urine, but sometimes their large size or irregular shape make it impossible to expel them. Sometimes the stones are so large that they cannot pass from the kidneys to the ureters, other times they are smaller, pass into the ureters but cannot travel through them; in these situations, appropriate therapies are necessary.
The chemical composition of the stones depends on the chemical imbalance in the urine. The four most common types of stones contain calcium, uric acid, struvite and cystine.
Calculi containing calcium constitute 85% of all kidney stones. The most common cause is the increase of calcium in the urine (hypercalciuria). Normally the excess calcium in the blood is removed by the kidneys which expel it with the urine. In situations of hypercalciuria, excess calcium builds up in the kidneys and in the urine and forms aggregates with other substances generating calculi. Also low levels of citrate, high levels of oxalate and uric acid and an inadequate volume may cause urinary stone formation.
The most common types of Kidney stones are:
- Calcium oxalate stones. Calcium stones are formed by calcium chemically bound to oxalate (calcium oxalate) or to phosphate (calcium phosphate). Of these, calcium oxalate is the most common. The calcium phosphate calculi occur typically in patients with hormonal or metabolic disorders such as hyperparathyroidism and renal tubular acidosis.
Increased intestinal absorption of calcium (hypercalciuria by absorption), excessive levels of parathyroid hormone (hyperparathyroidism) and excessive filtration of calcium by the kidney (deficiency of the kidney to reabsorb calcium filtered) can cause hypercalciuria. Also states of prolonged inactivity can increase urinary calcium.
Renal tubular acidosis is a hereditary disease in which total levels of urinary citrate are significantly reduces, these factors can lead to stone formation, usually calcium phosphate. - Uric acid stones. The protein digestion produces uric acid, which is expelled with urine. In increased concentrations uric acid cannot dissolve in urine and therefore aggregates forming calculi. Genetic factors also affect, since uric acid stones are more common in men. Uric acid stones constitute about 10% of kidney stones.
- Struvite. Called also infectious calculi, develop when a urinary tract infection (for example, cystitis) alter the chemical balance of the urine. To encourage their proliferation, the bacteria produce chemical substances that neutralize acid in the urine, this mechanism underlies the formation of struvite stones. Struvite stones are more common in women because they are more frequently subject to urinary tract infections. These calculi usually form jagged structures and can reach a considerable size.
- Cystine stones. Cystine is an amino acid (a constituent of proteins) which, if present in excessive amounts, does not dissolve in urine. There is a rare inherited disorder in which high levels of cystine accumulate in the urine. This condition (called cystinuria) determines the formation of cystine stones, which are difficult to treat and require a life-long treatment.
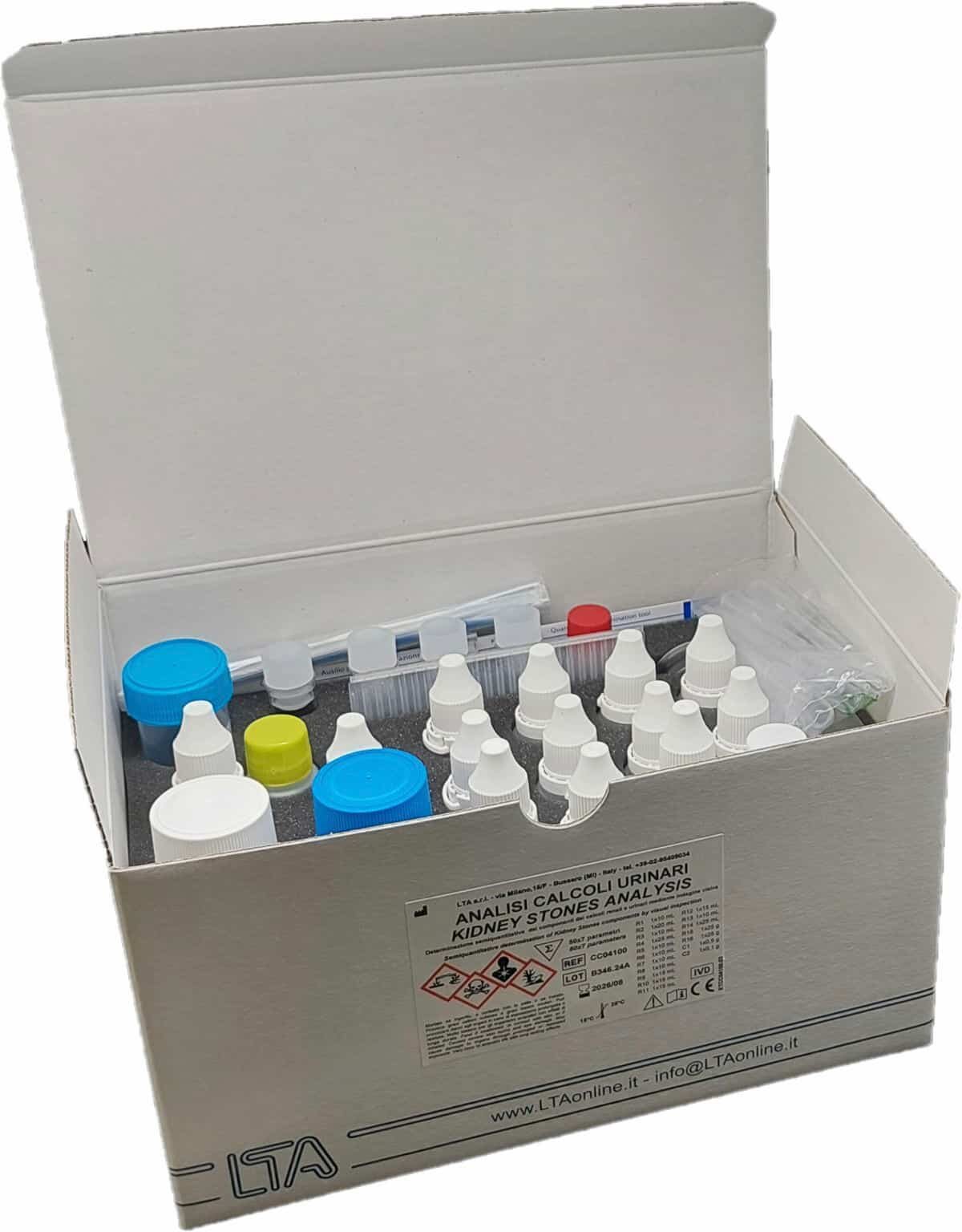
LTA kit for Kidney Stones Analysis is ready to use kit for the semi-quantitative colorimetric determination of carbonate, calcium, magnesium, ammonium, oxalate, phosphate, uric acid and cystine on kidney and urinary stones.

A small quantity of urinary (or kidney) stones is crushed and pulverized. On this sample, as homogenous as possible, the following semi-quantitative determinations can be carried out: calcium, magnesium, ammonium, oxalate, phosphate, uric acid and cystine.
Package contents:
(50 TESTS x 7 parameters)
16 Reagents to perform the test of the 7 parameters plus carbonates
2 Controls (Control 1 for Carbonate, Calcium, Magnesium, Ammonium, Oxalate, Phosphate, Uric acid and Control 2 for Cystine)
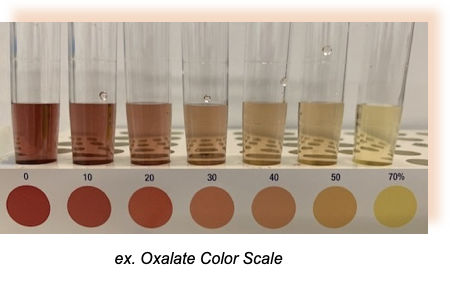
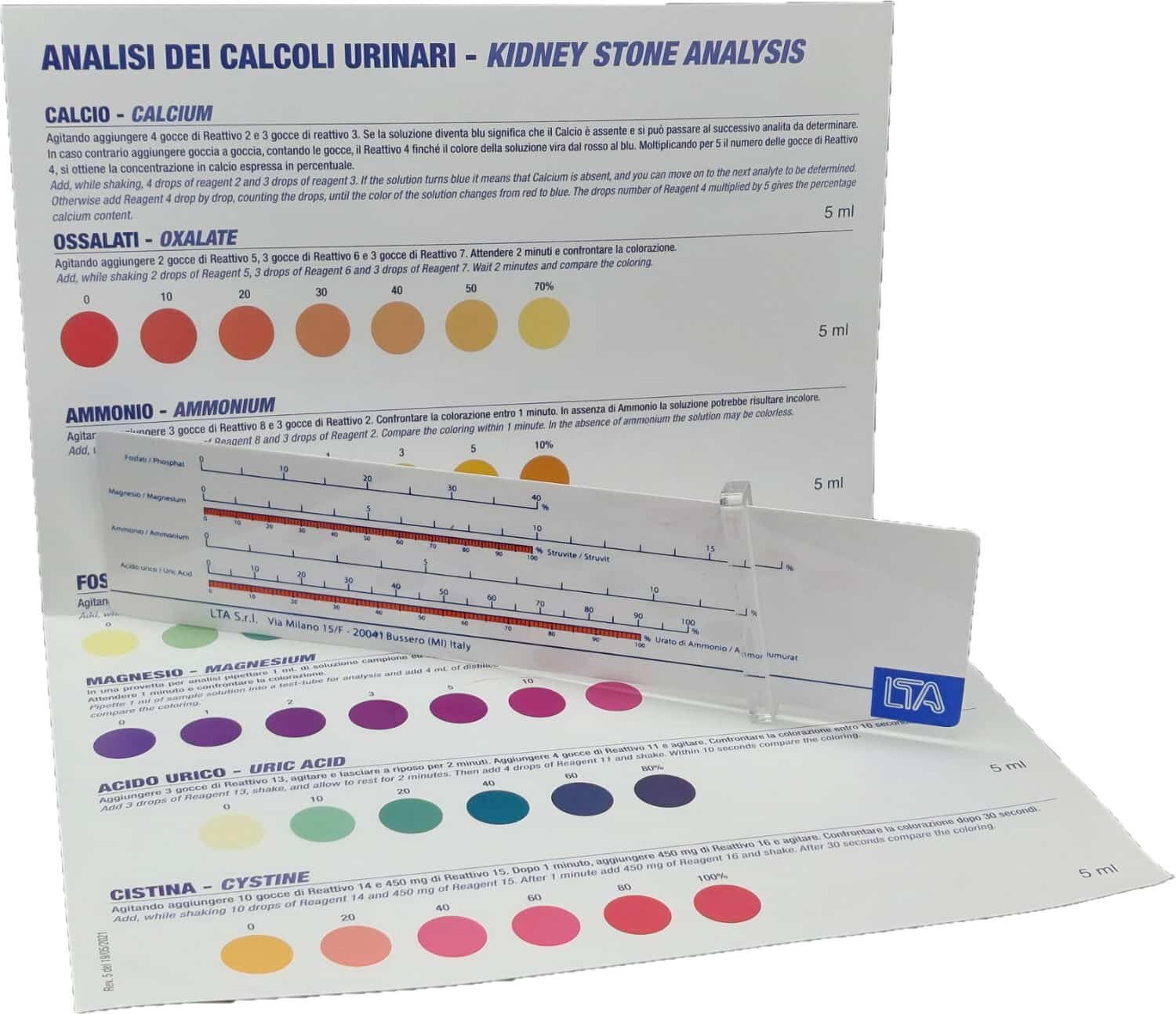
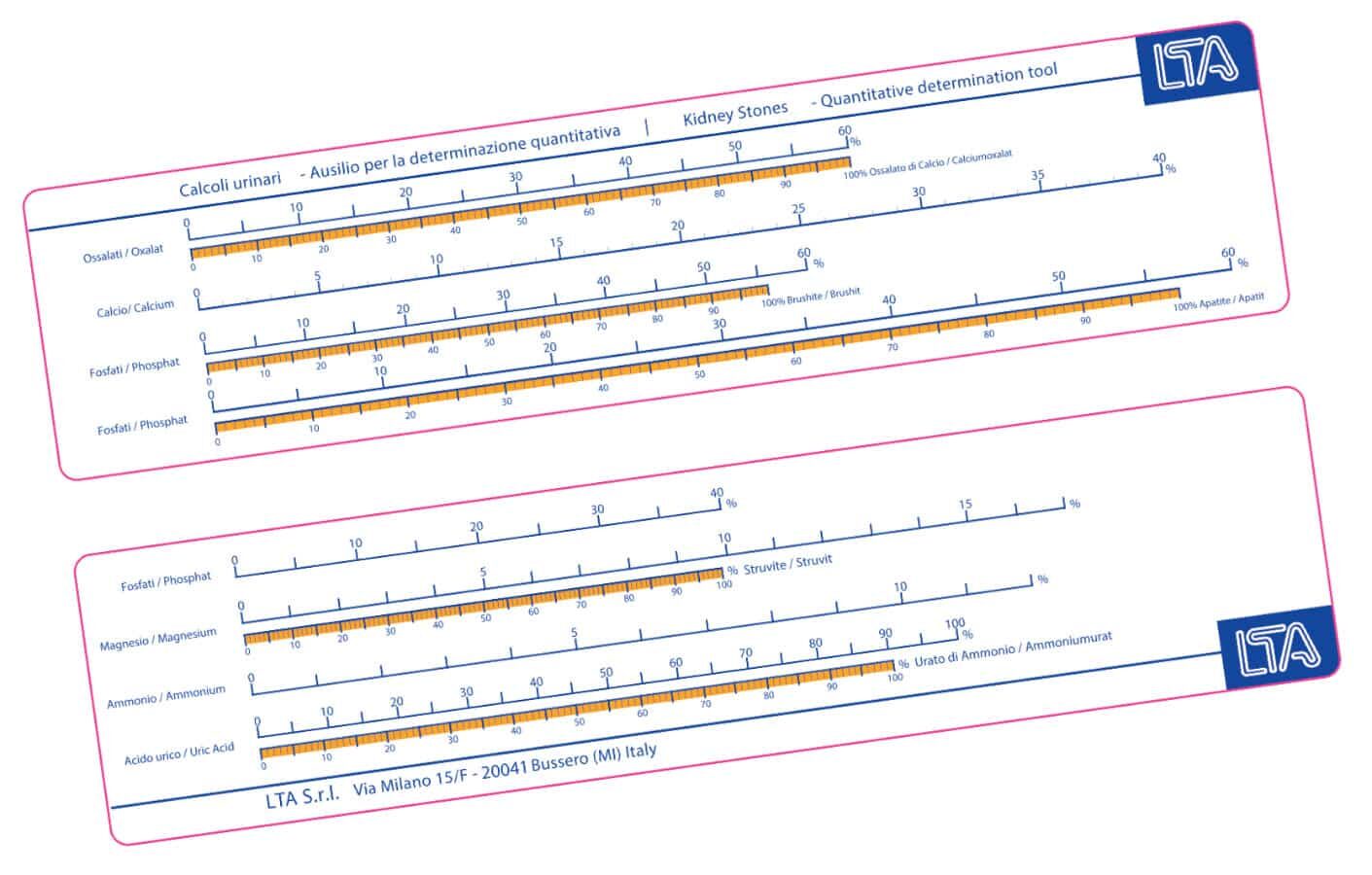
All the disposables needed to perform the tests + Color scale and Slide rule for the interpretation of the results.